Ask yourself one question: How do you want to survive?
General hospitals derive approximately 40% of their revenue from cardiovascular procedures. According to the 2016 Physician Inpatient/Outpatient Revenue Survey conducted by Merritt Hawkins, a physician practicing cardiology generates a net annual revenue of $2,448,136 for his or her respective facility. The reason may be obvious: cardiovascular disease (CVD) kills more people in the United States than any other cause, with cancer following closely in second place.
The western medical community has aptly found a way to cope with the prevalent problem of heart disease. It’s become common practice to treat the symptoms and aftermath, leaving the cause unaffected. Granted, thousands of lives are prolonged due to procedures like coronary artery bypass grafts (CABG), balloon angioplasties and coronary stents, but… isn’t there an easier way? Compare our rates of CVD to those of other developed countries and the monkey is left scratching his head. Further compare our healthcare costs with those same countries, and the paradox spirals further down into the abyss until an understanding is presented. There exists a modern-day gold rush in the healthcare industry, and the risk for developing CVD can be significantly lowered with a no-cost alternative: physical activity.

CVD is an all encompassing term with several major conditions falling under the umbrella, including coronary artery disease (CAD), chronic heart failure (CHF), primary hypertension and stroke. CAD is characterized by atherosclerotic deposits of plaque forming along the endothelial (internal) walls of the coronary arteries that nourish the heart. If an occlusion grows large enough it may lead to a myocardial infarction.
The fundamental driving force of the disease progress is inflammation. Many lifestyle-related choices contribute to a systemic inflammatory response, leading to the gradual onset of atherosclerosis and CAD. Smoking, physical inactivity, poor diet – all of these exacerbate the rate of vascular degeneration and stenosis. Compound the aforementioned habits with an unavoidable hereditary predisposition in some cases, and heart disease is potentially inevitable.
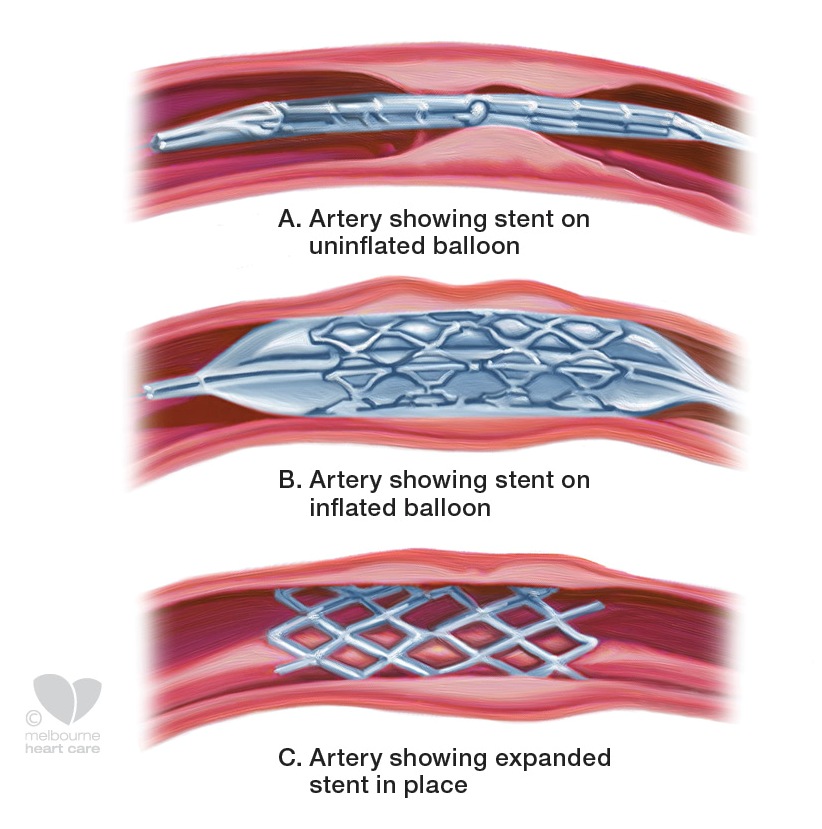
One of the most common procedures used to treat CAD is the emplacement of a coronary stent. A stent is a small, metal mesh tube that provides a reliable scaffolding, propping open a plaque-ridden artery. The result is improved blood flow to the heart and therefore, improved function. Thousands of lives are prolonged each year. Stenting is safer and easier than a bypass, however, it’s not a fix-all. If poor lifestyle habits remain, then many patients face follow-up procedures.
In 2003, the internationally-revered journal, Circulation, published an interesting article comparing the effects of a 12-month exercise intervention to the emplacement of a stent to treat CAD. The randomized trial included 101 men with stable CAD, all of whom qualified for a percutaneous coronary intervention (PCI) with stenting. The men were divided into two groups and either underwent a PCI with no changes to lifestyle, or were placed on a 12-month exercise program consisting of cycling and group exercise and received no stent.
Here are some of the major results:
- A significantly higher number of patients in the stent group had adverse cardiac events during the 12-month trial (21 events in 15 patients); the exercise group had 6 events in 6 patients. There was an overall higher, event-free survival rate for those that conducted physical activity and received no stent.
- Roughly 45% of the patients who received a stent had progression of CAD at the 12-month follow up, vs. 32% of the patients in the exercise group.
- There was no change in the diameter of the targeted artery for those in the exercise group, yet they had a significant (16%) improvement in aerobic capacity, a significant decrease in resting heart rate, and significant improvement in total work capacity compared to the PCI group.
- A 31% decrease in diameter of the stented arteries was noted after 12 months (remember, no change was seen in either direction in the exercise group), yet there were no significant changes in aerobic or work capacity, nor resting heart rate.
Economically, the exercise intervention was the cheaper option. The total average healthcare cost of lifestyle modification was about half (average of $3,708) compared to the procedural strategy ($6,086), taking into account the significantly higher number of adverse events in the stent group, training facilities and equipment. Yet, we still get sucked into the invasive fix.
Someone Is Getting Rich
All that being said, the use of stents as a treatment for CAD has been under scrutiny. Questions have been raised regarding the overuse of stenting by physicians, i.e. the devices being selected as a go-to for patients that stand to gain little or no benefit from the procedure. Both the Joint Commission and the American Medical Association have published documentation illustrating the unforeseen dangers of conducting unnecessary angioplasties. Many nationally-published media outlets, such as Bloomberg, The New York Times, and US News, have relayed the controversy to the public, however, not much has changed. Patient anxiety may be a driving force – to find out your risk of death increases due to an occluded artery will instill an underlying panic to survive, and stent emplacement is the quickest fix possible. However, what exists that is often more powerful than individual human ethics? Lucrative practices.
- What is the average cost of a cardiac stent? Enter: Healthcare Bluebook – an amazing collection of data considering the convolution that exists when comparing hospital billing strategies in the US. Founded by Jeff Rice, MD, their mission is to provide transparency to consumers in the realm of healthcare. After combing the website, as well as PubMed, their rates seem legitimately founded on accurate figures, therefore, the information presented here has been derived from their database. According to HBB, a “fair price” for a full, in-patient procedure is $27,007. They go on to note, “The most expensive [care] can cost more than five times as much as providers that charge a Fair Price.” This means upwards of $135,000.
- How many procedures are conducted a year? Roughly 600,000 procedures are conducted each year. One procedure does not necessarily mean one stent. The surgeon may sometimes emplace 2 or 3 stents depending on the needs of the patient. This partially weighs into the range of costs mentioned in Step 1, above.
- Total cost: $27,007 x 600,000 procedures = $16.2 billion annually. Roughly one-half of the procedures are Medicare patients.
- According to Merritt Hawkins, the average salary of an invasive cardiologist is $525,000.
- Becker’s Hospital Review reported the average base salary of an independent hospital CEO at $421,800, and an average total cash compensation of $479,700. Subsidiary hospital CEO figures were reported to be slightly less.
- The American Hospital Association lists 5,627 registered hospitals, with an annual net revenue of $151.9 million per hospital.
In 2013, TIME Magazine dedicated an entire issue to a 2-year investigation into hospital billing. The story, Bitter Pill: Why Medical Bills Are Killing Us, deserves applause – a representation of how good journalism should be. The ambiguity between hospital costs stems from markup beyond baseline, government-determined Medicare rates – from astronomical markups on simple things like acetaminophen pills ($1.50 per pill at a hospital… $1.49 for 100 tablets on Amazon.com), X-rays ($20.44 according to Medicare… $283.00 at MD Anderson Cancer Center in Houston, TX) and, of course, more complex services like cardiovascular bypasses and stents.
Drs. Frank Booth, Christian Roberts and Matthew Laye composed a lengthy research article diving into the concept of physical inactivity as a primary cause for chronic disease. The article, Lack of Exercise is a Major Cause of Chronic Diseases, investigates the role of physical activity as a primary prevention strategy for 35 chronic conditions, and discusses how sedentary time alters favorable biological and genetic adaptations that would otherwise exist in healthy, exercising individuals. Large reductions in risk for developing CVD exist in individuals who regularly exercise, upwards of 50%. Things a stent can’t do? A stent cannot influence favorable changes in blood pressure, inflammatory markers and HbA1c, vascular tone, antioxidant and nitric oxide levels, aerobic exercise capacity, longevity… the list goes on.
Now, breathe and repeat the question: How do you want to survive?
References:
Booth, F. W., Roberts, C. K., & Laye, M. J. (2012). Lack of exercise is a major cause of chronic diseases. Comprehensive Physiology, 2:1143-1211
Hambrecht, R., Walther, C., Möbius-Winkler, S., Gielen, S., Linke, A., Conradi, K., … & Sick, P. (2004). Percutaneous coronary angioplasty compared with exercise training in patients with stable coronary artery disease a randomized trial. Circulation, 109(11), 1371-1378.
Hello there! Do you use Twitter? I’d like to
follow you if that would be okay. I’m absolutely enjoying your blog and look forward to new
posts.
Unfortunately I am not on Twitter, however truPhys is on Facebook @turphys if you use that. Thanks for the feedback, I’m glad you enjoy what you’re reading!!
Pingback: 6 Ways Mountain Bikes Are Winning Big and Changing the World - Singletracks Mountain Bike News